Updated March 9, 2009
Please note that Dr. Semple does not endorse nor advocate the use of any products advertized by Angelfire on this site. The only therapies that are "proven" to help patients with ITP are those that have undergone the scutiny of prospective randomized controlled clinical trials. Herbal formalas and many other products HAVE NOT been "proven" to help patients with ITP. Anyone that sells them with claims that they help or cure ITP are simply trying to get your money. PLEASE BEWARE.
I am also a member of the Toronto Platelet Immunobiology Group
(affectionately known as TPIG).
Its a network of scientists and physcians which are committed to transfusion immunology research.
We are also active in disseminating information about immune blood cell disorders. The
group has close links with the
Hospital for Sick Children, and the
Canadian Blood Services.
Our research is in the area of platelet immunology. We primarily study the
pathogenic immune mechanisms responsible for autoimmune (e.g. ITP or AITP) and alloimmune
(e.g. transfusion-induced) platelet disorders and the mechanism of action of established clinically "proven"
therapies such as IVIg and anti-D. Related to these areas, we also attempt to develop novel
and safe immunotherapeutic approaches to specifically down-regulate platelet antibodies.
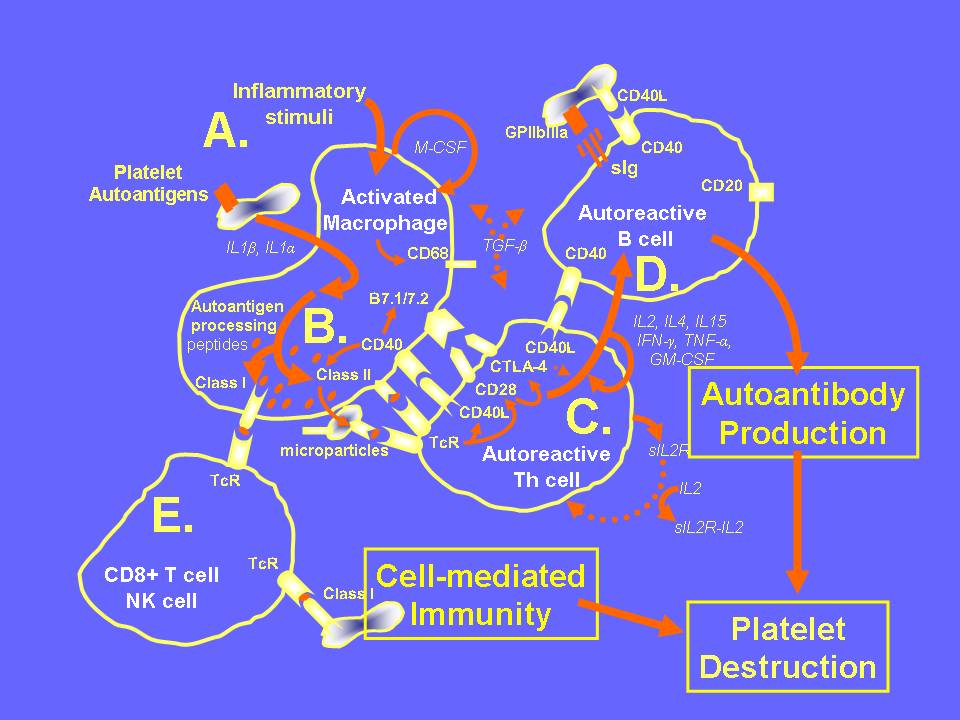
If we were to summarize the majority of the scientific literature regarding the immune pathogenesis of AITP, it might paint the following picture:
It appears that the major autoimmune stimuli initiating AITP occur at the APC-Th cell synapse. Collectively, these data support the need for clinical trials relating to T cell and APC modification in AITP(e.g. GPIIbIIIa peptide therapy etc.).
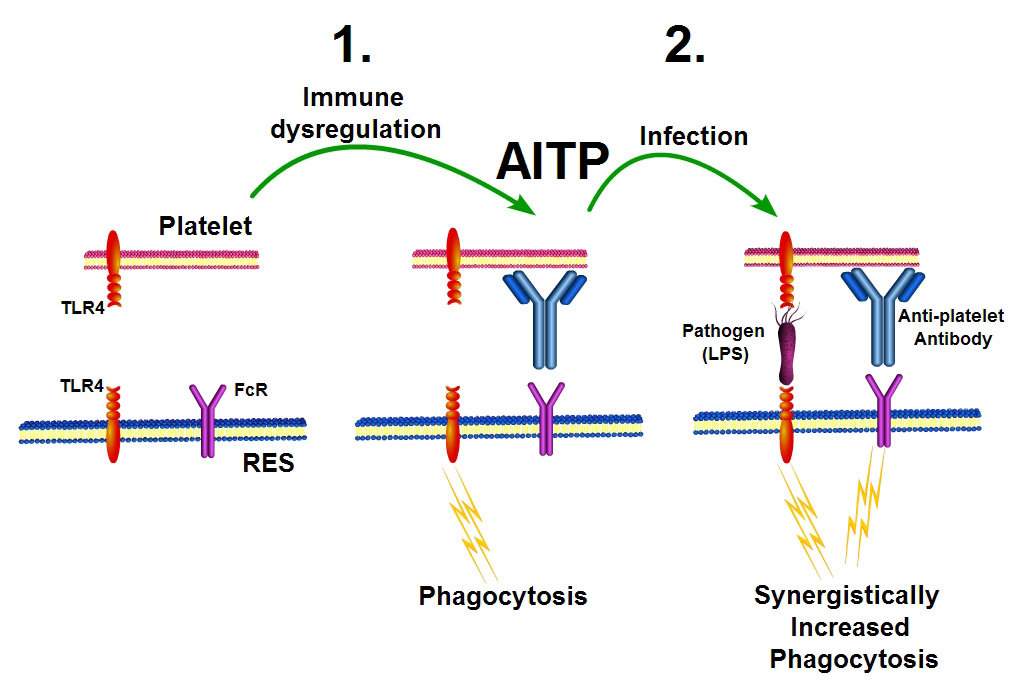
Our most recent studies suggest that platelets' express Toll-like receptors (particularly TLR4) and act as circulating sentinals to sence infections (Aslam et al Blood 2006). TLR expression on platelets also appears to significantly affect platelet destruction, especially when platelets are opsonized with anti-platelet antibodies (Semple et al Blood, 2007). These mechanisms may be the reason why thrombocytopenia worsens in some patients with AITP during infections and, alternatively, resolves in other patients with AITP who are treated with bacterial eradication therapy. This is summarized in the following diagram:
1. Immune dysregulation leads to the production of anti-platelet autoantibodies, RES phagocytosis and thrombocytopenia. 2. When some ITP patients become infected e.g with bacteria (containing LPS), their platelet destruction worsens and even more platelets are destroyed (counts drop further). If the infections is eradicated, the platelet destruction is relieved and platelet counts can rise.
On the other hand, for allogeneic platelet transfusions, our results in mice suggest the following immune mechanisms are involved:
Our current research efforts focus on the following projects:
Anti-platelet T cell responses in children with acute and chronic autoimmune
thrombocytopenic purpura (AITP).
Analysis of platelet- and GPIIbIIIa-reactive T helper cell lines and clones derived
from patients with chronic autoimmune thrombocytopenic purpura (AITP).
The role of anti-inflammatory mediators in controlling humoral and cellular immune
responses in recipients receiving platelet transfusions.
The antigen processing and presentation pathways of platelet allo- and auto-antigens
within macrophages.
The ability of platelets to mediate innate immune mechanisms via TLR.
The mechanism of action of novel intravenous gammaglobulin(IVIg) and anti-D preparations
in modulating platelet-induced immunity.
If you would like more information on these subjects then feel free to email me
at: semplej@smh.toronto.on.ca
The following sections outline more details of the lab's activities
Post-doc, grad student and current employment information
Selected Publications:
Kjeldsen-Kragh J et al. Haematologica. 94(3):441-443, 2009.
Semple JW et al. Transfusion 48(9):1917-1924, 2008.
Aslam R et al. Transfusion 48(9):1778-1786, 2008. (Featured in an editorial)
Semple E et al. J Oral Maxillofac Surg. 66(4):632-638, 2008.
Ofosu F et al. Thromb Haemost 99(5):851-862, 2008. (Review)
Semple et al. Vox Sang 3(1):152-158, 2008. (Review)
Semple JW Blood 112(4): 927-928, 2008. (Inside Blood)
Semple JW. Thromb Haemost 99(2), 249, 2008. (Editorial)
Aslam R et al. Transfusion 47(11): 2161–2168, 2007.
Cognasse F et al. Current Immunol Rev 3:109-115, 2007 (Review)
Semple JW. Eur J Heamtol 79(4):279–280, 2007 (Editorial)
Semple JW. Blood 110(8), 2784-2785, 2007, (Inside Blood)
Aslam R et al Transfusion 47:2161, 2007
Kjaersgaard M et al Blood 110:1359, 2007
Semple JW et al Blood 109:4803, 2007
Semple JW et al Drug Discovery Today 3:231, 2006
Aslam R et al Blood, 107:637,2006
Semple JW et al Sem Hematol 42:122, 2005
Sayeh E et al Blood 103:2705, 2004
Sayeh E et al Transfusion 44:1572, 2004
Coopamah MD et al Blood 102:2862, 2003
Coopamah MD et al Transfusion Medicine Rev 17:69, 2003
Semple JW et al J Pediatr Hematol Oncol 25 (Suppl 1), 11S, 2003
Semple JW et al Transfusion 42:958, 2002 (COVER ARTICLE - See above)
Semple JW et al Blood 100:1055, 2002
Semple JW et al Amer J Hematol 69:225, 2002
Post-Doctoral Fellows and Graduate Students:
My lab has an active training program for post-doctoral fellows and graduate students
who are interested in pursuing studies related to transfusion immunology.
To apply for a post-doctoral position, please send your CV and a brief summary of research
accomplishments to me at the above email address.
If you are interested in pursuing graduate studies in my lab (e.g. MSc or PhD), you need to be first accepted by the School of Graduate Studies at the University of Toronto. For more information about U of T. admission requirements, follow the following links: